Human Immunodeficiency Virus Infection
Approximately 36 percent of AIDS cases diagnosed in 1992 were attributable to intravenous drug abuse. It is estimated that drug abuse-related HIV and AIDS cases cost $3.7 billion.
Synopsis
The CDC monitors the incidence and prevalence of AIDS cases by risk category. To date, approximately 35 percent of all AIDS cases originated with an intravenous drug user (IVDU). About 36 percent of the cases reported in 1992 to the CDC originated with an IVDU. This rate is applied to the total annual cost of treating HIV/AIDS estimated for 1992 (or $10.3 billion spent for inpatient, outpatient, pharmaceutical, long-term care, and home-health services). Approximately 20 percent of the direct medical costs for all persons with HIV and AIDS are covered by Federal and State Medicaid programs. In addition to private insurance, the remaining direct medical costs are covered by other public subsidies and indigent care funds.
These estimates may be conservative, however, because IVDU's are likely to be more dependent on the public health care system than other patients. Because many IVDU's lack insurance or private funding to cover medical expenses, the burden on the health care system will increase as the percentage of IVDU-related HIV cases continues to rise. Finally, this study allocates all HIV/AIDS costs to drug abuse because of the connection with intravenous drug use. However, alcohol may also play a role in transmission of HIV/AIDS by impairing drinkers' judgment and increasing their proclivity to take risks - such as engaging in unprotected sex.
Relationship Between Intravenous Drug Use and Human Immunodeficiency Virus
Intravenous drug users contract HIV primarily by sharing contaminated needles. Using data supplied by the CDC, this study estimates that 36 percent of HIV infections in 1992 were attributed to intravenous drug use (CDC 1993a). This includes infections of other IVDU's as well as their sexual partners and children. As of September 1993, there were 11,750 reported AIDS cases among women who had sex with IVDU's and 2,766 pediatric AIDS cases in which the mother was an IVDU or had sex with an IVDU. Since the first AIDS case was reported in 1981, 51 percent of the heterosexual and pediatric transmission cases have been related to intravenous drug use. Many of these cases have involved women who exchange sex for drugs.
The National Institute on Drug Abuse estimates that there are 1.1 to 1.3 million IVDU's in the United States and its territories (Schuster 1988). According to the 1992 National Household Survey on Drug Abuse, however, these numbers may be an underestimate because 660,000 persons in households reported intravenous drug use within the past month and 3 million reported use during their lifetimes. The survey is frequently criticized as an underestimate because it does not cover the more than 1 million prisoners (U.S. Department of Justice 1993a) or 500,000 to 650,000 homeless persons who are IVDU's (Burt and Cohen 1989). Most IVDU's are on the East Coast, with the largest concentration (250,000) reported in New York City. Because of the transient nature of this population, however, accurate estimates are difficult to make.
The Human Immunodeficiency Virus Epidemic
According to the most recent Public Health Service estimates, approximately 1.0 to 1.5 million persons are infected with HIV (CDC AIDS Hotline 1994, personal communication). The incidence of HIV/AIDS grew dramatically from 1985 to 1993, although part of the increased incidence is attributable to major expansions in the definitions of AIDS that were put into effect in 1993. However, since that time, the number of new AIDS cases reported each year has declined. Through 1992, the cumulative number of AIDS cases attributed to intravenous drug use exceeded 68,000.
From 1987 to 1992, the number of newly reported HIV/AIDS cases associated with intravenous drug use increased from 27 percent to 36 percent of the total number of cases. In 1992, an estimated 36 percent of newly reported AIDS cases were drug related (17,115): 25 percent of the total cases were IVDU's (11,738); 6 percent were homosexual IVDU's (2,869); 4 percent were sex partners of IVDU's (2,130); and less than 1 percent were pediatric cases where the mother was an IVDU or a sex partner of an IVDU (378). More than 54 percent of all heterosexual transmission cases and 52 percent of all pediatric transmission cases involved sexual partners of IVDU's (CDC 1993a; figure 4.3 below).
Costs of Treating Patients Infected With Human Immunodeficiency Virus
During the past decade, the total direct costs of treating all persons who are HIV positive have increased dramatically. Estimates have ranged from $630 million in 1985 (Scitovsky and Rice 1987) to $3.3 billion in 1989 (Hellinger 1990) to $5.8 billion in 1991 (Hellinger 1991). The total cost of treating all persons who are HIV positive is estimated to have been $10.3 billion in 1992 (Hellinger 1992). This number may be inflated, however, because of a $20,000 decrease in treatment cost estimates from 1992 to 1993 (Hellinger 1993). With approximately 36 percent of all HIV infections attributed to intravenous drug use, the total direct costs attributed to drug abuse were $3.7 billion. However, these figures may underestimate the cost of treatment for IVDU's. IVDU's are likely to be more dependent on the health care system for services than other persons. Not only are IVDU's generally sicker when they enter the system, but they are also less likely to have a support network of family and friends (Nichols 1989). Without a strong support network, IVDU's are more likely to use hospital and other home-health care services, resulting in higher direct medical costs.
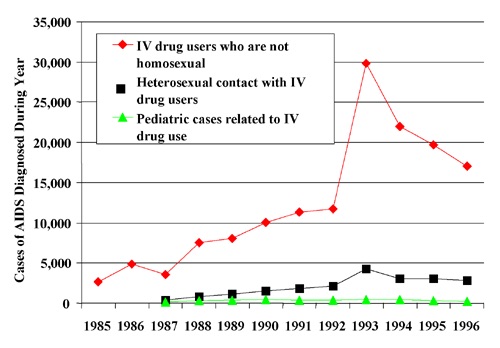 Figure 4.3 Number of Persons Diagnosed With AIDS by Intravenous Drug-Related Risk Group, by Year of AIDS Diagnosis, 1985-1996
Figure 4.3 Number of Persons Diagnosed With AIDS by Intravenous Drug-Related Risk Group, by Year of AIDS Diagnosis, 1985-1996Source: CDC, HIV/AIDS Surveillance, year-end editions, 1993-1997.
Several studies were conducted to estimate the cost of treating a person with AIDS. Estimates of lifetime treatment costs have ranged from $70,000 in 1985 (Scitovsky and Rice 1987) to $147,000 in 1985 (Hardy et al. 1988) to $140,000 in 1992 (Hellinger 1993). Hellinger (1993) estimated that the annual cost of treating an individual from the onset of infection to death was $119,274. These costs have decreased during the years as new treatments and therapies have been successful in transforming HIV from an acute illness that necessitates frequent hospitalizations to a chronic illness with long periods of low-intensity care and fewer hospitalizations.
To understand the full impact of the direct medical costs of AIDS on the health care system, the total costs from the onset of HIV infection to death must be computed. The cost of treatment can be broken down into four phases: Phase 1 represents persons who are asymptomatic, phases 2 and 3 primarily represent persons who are symptomatic, and phase 4 represents persons with AIDS.
For each phase of HIV infection, Hellinger estimated the monthly cost for inpatient, outpatient, home-health, drug, and long-term care costs. Monthly costs were derived by multiplying the average length of stay, average number of hospitalizations, and average cost per day. The increase in treatment costs as the disease progresses through phase 4 is a reflection of the higher proportion of inpatient episodes (i.e., increases in the average length of stay and average number of hospitalizations) (see table 4.17).
According to the AIDS Cost and Service Utilization Survey data, the average total time from HIV infection to death is 149 months or 12.4 years, with a survival time for phase 4 of 25 months (Hellinger 1993). By multiplying the mean duration of each phase by its respective total cost per month, the estimated total lifetime cost of care for a person infected with HIV is $119,274 (see table 4.18).
As previously indicated, direct medical expenditures for the treatment of HIV and AIDS attributed to drug abuse are substantial. However, other "indirect" medical costs also add to the economic burden the epidemic is placing on the health care system. For example, the American Red Cross currently screens all 12 million donated units of blood for HIV antibodies (Wallace et al. 1993). In addition, more indirect medical costs arise as practitioners and other health care personnel take extensive precautions to avoid infection through contamination by HIV-positive blood.
IVDU's are highly dependent on public insurance and indigent care to fund medical expenses associated with treatment for HIV infection and AIDS. Hellinger (1993) reported that overall, approximately 40 percent of all AIDS patients receive Medicaid payments during some part of their illness. Federal and State Medicaid expenditures for treating persons with AIDS were approximately $2 billion in 1992, while Medicare expenditures were $280 million (Hellinger 1993).
Scitovsky (1991) found that the degree to which the Government subsidizes treatment for AIDS is most evident in public hospitals, where 83 percent of all AIDS admissions are Medicaid or self-pay. Hospitals frequently provide "free care" to persons who have no insurance or funds to cover the expenses. Based on a nationwide survey of AIDS patients at acute care hospitals, the average loss at public hospitals per AIDS patient was $5,818 (1987 dollars) per year. Since IVDU's and sexual partners of IVDU's are less likely to have private insurance than other patients with HIV infection, the uncompensated care burden on both public and private hospitals is substantial.
Hepatitis B and Hepatitis C Infection
Drug abuse-related behaviors are estimated to cause 12 percent of hepatitis B (HBV) cases and 36 percent of hepatitis C (HCV) cases each year. The cost of treatment for drug abuse-related HBV and HCV cases in 1992 is estimated to be $462.4 million.
Synopsis
In 1992, approximately 200,000 to 300,000 new acute hepatitis B (HBV) infections and 170,000 new acute hepatitis C (HCV) infections occurred. Using these estimates, the total estimated cost for treating acute HBV and HCV cases was almost $271.5 million and almost $1,193.8 million, respectively. Approximately 12 percent of HBV and 36 percent of HCV cases diagnosed during 1993 were related to intravenous drug abuse. Accordingly, the estimated cost of drug abuse reflected by HBV and HCV treatment is $32.6 million and $429.8 million, respectively, for a total of $462.4 million in 1992.
The much greater cost for HCV infection is because more cases of HCV infection become chronic than is the case with HBV (50 percent compared with less than 10 percent). If current trends continue and the incidence and prevalence of HCV continues to rise, the burden on the health care system will increase because 50 percent of persons who contract HCV are predicted to experience long-term, chronic health problems.
Hepatitis B and Hepatitis C Virus
The annual number of HBV cases reported to CDC has decreased since the early 1980's (see figure 4.4 below). The decrease, however, has been modest (38 percent since 1982) considering that a safe and effective vaccine for HBV was introduced in the United States in 1981. CDC annual infection estimates are derived using a factor based on a comparison of active versus passive surveillance of HBV and HCV cases (Alter et al. 1987; CDC 1993c, personal communication). In 1992, there were 16,126 new HBV cases reported to the CDC. According to the most recent CDC estimates, approximately 200,000 to 300,000 new acute HBV infections occur annually. More than 50 percent of new acute cases are asymptomatic (CDC 1993c, personal communication).
Approximately 6 to 10 percent of persons older than age 5 who contract acute HBV each year become chronic carriers (CDC 1993c; Sherlock 1987). Chronic carriers are defined as persons who are seropositive for HBsAg (hepatitis B surface antigen) for more than 6 months (Sherlock 1987). Chronic carriers can either remain "healthy" or develop various forms of chronic hepatitis, cirrhosis, or primary hepatic cancer. These numbers are inversely proportional to age, as the risk of chronic infection for infants who acquire infection during the prenatal period is 70 to 90 percent (Shapiro 1993). Males with acute HBV infection are also six times more likely than women to become chronic carriers (Sherlock 1987). Roughly 1 million persons are chronic carriers of the HBV (CDC 1993c).
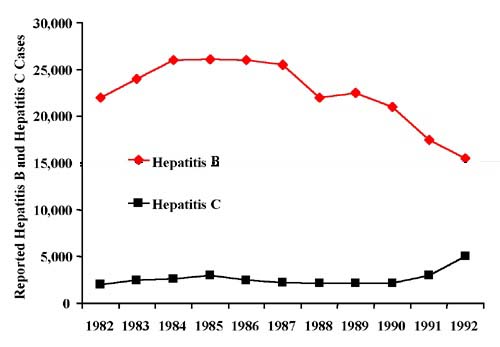 Figure 4.4 Reported Hepatitis B and Hepatitis C Cases, 1982-1992
Figure 4.4 Reported Hepatitis B and Hepatitis C Cases, 1982-1992Source: CDC (1993b) Note: The HCV numbers were derived from the number of non-A, non-B hepatitis (NANB) cases reported to CDC. Approximately 80 percent of NANB cases are HCV.
In contrast to HBV trends, the number of reported HCV cases has been increasing during the past several years (see figure 4.5 below). As with HBV, annual incidence estimates are derived by extrapolating the total number from the actual number of HCV cases reported to the CDC. According to the most recent CDC estimates, 170,000 new infections occur annually (CDC 1993c). Approximately two-thirds of all acute HCV cases are either asymptomatic, mild, or hard to detect (National Hepatitis Detection and Treatment Program 1991). Acute episodes of HCV are generally less severe than acute episodes of HBV. In contrast to HBV, approximately 50 percent of acute HCV cases (85,000) become chronic.
The most common mode of infection for HBV is sexual contact, with intravenous drug use and perinatal transmission accounting for the majority of the remaining reported cases in which risk was identified. As seen in the AIDS epidemic, the proportion of total HBV cases involving heterosexual contact is rising, while the number of cases reported through homosexual transmission is decreasing (CDC 1993c). This trend appears to be associated with behavior modification among homosexual men in response to the AIDS epidemic. From 1981 to 1987, the number of reported cases of HBV through intravenous drug use increased 77 percent (Bloom et al. 1993). However, over the past several years, the percentage of HBV cases attributed to intravenous drug use has decreased from between 24 and 29 percent in the mid-1980's to 12 percent in 1993 (Alter et al. 1990b; CDC 1993c).
HCV is most commonly transmitted through intravenous drug use and blood transfusions and is rarely acquired through sexual contact. In contrast to the epidemiological trends of HBV, the proportion of reported HCV cases acquired through intravenous drug use remains very high (12 percent versus 36 percent, respectively). The risk of acquiring HCV through intravenous drug use also increases as the duration and frequency of drug use increases. According to an Australian study, approximately 66 percent of IVDU's acquire HBC within 2 years of regular intravenous drug use, and virtually 100 percent of IVDU's acquire HCV within 8 years of regular use (Bell 1990). The results of this study, however, should be used with caution because characteristics of IVDU populations (such as needle sharing) have been shown to vary across and within countries.
HBV has been identified as a major cause of cirrhosis and primary hepatic cancer. Associations between HCV and primary hepatic cancer have also been identified. For example, between 20 to 40 percent of persons with chronic HCV will develop cirrhosis (National Hepatitis Detection and Treatment Program 1991). Although many persons with cirrhosis do not exhibit symptoms initially, there is a high mortality rate due to eventual hepatic decomposition. Beasley (1988) reported that persons with cirrhosis are more likely than carriers or persons with chronic active hepatitis to develop primary hepatic cancer. Beasley also noted that international studies have shown that HBV is a major etiologic agent for primary hepatic cancer in 75 to 90 percent of cases.
Relationship Between Intravenous Drug Use, HBV, and HCV
IVDU's contract HBV and HCV by sharing contaminated needles. Studies have shown that IVDU's are at high risk to acquire HBV and HCV, as seroprevalence rates range from 65 to 90 percent (Bailly 1989; Piot et al. 1990). During 1993, 12 percent of HBV infections (Shapiro 1993) and 36 percent of HCV infections were attributed to persons who use intravenous drugs (CDC 1993c). These estimates may be conservative, because at least 30 percent of adults who reported HBV and HCV cases did not specify a risk factor (Shapiro 1993; CDC 1993c). It is possible that some persons with unidentifiable risk factors were reluctant to identify intravenous drug use as a risk factor.
As in HIV infection, IVDU's infect not only other IVDU's but also their sexual partners. Transmission of HBV through heterosexual activity has been increasing each year, and perinatal transmission of HBV by mothers who use intravenous drugs or have sexual intercourse with an IVDU is common, with transmission rates reaching 90 percent (Arevalo and Washington 1988). Sexual and perinatal transmission of HCV is rare, however (Piot et al. 1990).
The public health concerns regarding HBV and HCV are justified. NIDA estimates from the 1992 U.S. Household Survey on Drug Abuse indicate that 660,000 persons reported intravenous drug use within the month preceding the survey and 3 million persons reported use during their lifetimes (SAMHSA 1993b). The survey does not cover the more than 1 million prisoners (U.S. Department of Justice 1993a) or 500,000 to 650,000 homeless persons (Burt and Cohen 1989). Most IVDU's are believed to be on the East Coast, with the largest concentration (250,000) reported in New York City (Jaffe 1992). Because of the transient nature of the IVDU population, however, it is difficult to make reliable estimates.
Costs of Treating Patients Infected With Hepatitis B and Hepatitis C
The cost of treating HBV reported by Bloom et al. (1993) is used in this report to estimate per- case treatment costs resulting from intravenous drug abuse-related HBV and HCV cases. The study builds cost estimates from the expected course of HBV during its acute phase (experienced by all cases) and the chronic phase (experienced by a small proportion of all cases). Bloom's estimates, reported in 1989 dollars, were inflated to 1992 dollars using the medical care component of the consumer price index (CPI) (see table 4.19). Data were not available on the average cost for treating an acute HCV case; accordingly, the HBV cost estimates were also applied to HCV (see table 4.20). However, it is clear that acute cases of HCV are more serious than HBV, suggesting that application of the HBV costs to HCV may underestimate the actual value of services provided to HCV victims.
Using these estimates, the total estimated cost for treating acute HBV and HCV cases was almost $271.5 million and almost $1.2 billion, respectively. If intravenous drug abuse caused 12 percent of the HBV cases and 36 percent of the HCV cases, then the cost of drug abuse reflected by HBV and HCV treatment is $32.6 million and $429.8 million respectively, for a total of $462.4 million in 1992. The much greater cost for HCV infection is due to the fact that more cases of HCV infection become chronic than is the case with HBV (50 percent compared with less than 10 percent).
Psychiatric Comorbidity
Synopsis
These preliminary estimates suggest that the cost of treating alcohol and drug abuse-induced psychiatric disorders in 1992 may have been as high as $3.06 billion. This amount accounts for 9.5 percent of total expenditures for specialty sector mental health care in 1992. Of the $3.06 billion, $1.92 billion was spent on mental health disorders attributed to alcohol abuse and $1.14 billion on mental health disorders attributed to drug abuse. These estimates have not been included in totals of this report because of the limited amount of research and data on this issue. The estimates have been calculated, however, to demonstrate the plausible order of magnitude of such costs and to highlight the importance of further research.
The $3.06 billion estimate was derived in a two-step process: first, estimating the number of cases attributable to alcohol and drug abuse and second, applying an average cost. One-half of the number of comorbid cases (i.e., cases in which a patient is diagnosed as having a primary mental disorder with a secondary alcohol or drug use disorder) in mental health treatment settings was used for the number of episodes. The average cost per case for the setting of care was then calculated and applied to the estimated case count by setting of care. Prior studies have estimated that on average, 5 percent of patients in specialty mental health settings have a primary alcohol and drug abuse/dependence diagnosis, for which they are presumably receiving primary alcohol and drug abuse treatment. Based on a review of the comorbidity literature, this study finds that it is plausible that one-half the remaining comorbid admissions in mental health (after netting out the primary alcohol and drug abuse treatment cases) may have been caused by alcohol and drug abuse.
There has been recognition that a significant number of people presenting to specialized mental health providers have a primary diagnosis of alcohol and drug abuse. However, the economic implications of large numbers of persons with primary mental health diagnoses who also have alcohol or drug abuse problems have received little analysis or acknowledgement.
A review of the literature finds a dearth of research on the nature and direction of the relationship between mental disorders and alcohol or drug abuse. Some limited studies find evidence that particular patterns of alcohol and drug abuse (types of substances) may contribute to or cause certain mental disorders (and vice versa). These mental health disorders can be temporary or long term in duration. Moreover, alcohol or drug abuse may exacerbate existing mental disorders, causing them to worsen to the point that people must seek mental health care.
The limited research into psychiatric and alcohol and drug abuse comorbidity has concluded that both mental health and alcohol or drug abuse treatment settings must address comorbidity in their client populations and recognize the relationship between the two co-occurring disorders. Mental health and alcohol and drug abuse treatment systems need to be working toward treating both disorders.
Prevalence of Comorbid Psychological and Alcohol and Drug Abuse Disorders
Comorbidity in General Population
This section of the study defines psychiatric comorbidity as a condition of an individual who simultaneously has one or more mental disorders plus an alcohol or drug abuse disorder. The prevalence of psychiatric comorbidity in the general U.S. population has been found to be higher than previously thought (Kessler et al. 1994). The two major data sets that focus on comorbidity are the National Comorbidity Survey (NCS) and the Epidemiologic Catchment Area (ECA) Study. Although each study employed rigorous methods to detect psychiatric symptomatology or a disorder, neither study collected much information about the timeframes during which these symptoms occurred. For alcohol and drug use disorders, it is only possible to report, for example, that an individual had particular symptoms in the past year and not whether the disorders were present or whether they preceded other mental disorders. Moreover, while the ECA was not based on a nationally representative sample, it did look within communities at both the general population and clinical populations. The NCS employed a nationally representative sample.
The NCS found that almost 50 percent of respondents reported at least one lifetime DSM-III-R-defined psychiatric disorder. More than one-half of all lifetime disorders occurred in the 14 percent of the population who had a history of three or more comorbid disorders. Nearly 30 percent of respondents reported at least one disorder in the 12 months before their interviews. Fifty-six percent of the respondents with a history of at least one disorder had two or more disorders. The major burden of a psychiatric disorder in this sector of our society is concentrated in a group of highly comorbid people who constitute about one-sixth of the population (Kessler et al. 1994).
The ECA data showed that estimated U.S. population lifetime prevalence rates were 22.5 percent for mental disorders not associated with alcohol or drug abuse, 13.5 percent for alcohol dependence/abuse, and 6.1 percent for other drug dependence/abuse. Among those with an alcohol disorder, 36 percent had a comorbid mental disorder. The highest mental-addictive disorder comorbidity rate was among those with drug (excluding alcohol) disorders, with 53 percent of this population found to have a mental disorder (Regier et al. 1990).
Figure 4.5 (below) illustrates the number of persons affected by mental illness, alcohol, and drug abuse along with comorbid alcohol and drug abuse and mental health disorders in a 1-year period. In 1 year, 6.5 million people were affected by comorbid alcohol and drug abuse and mental illness disorders. These persons sought treatment in mental health and/or alcohol and drug abuse treatment settings (Narrow et al. 1993).
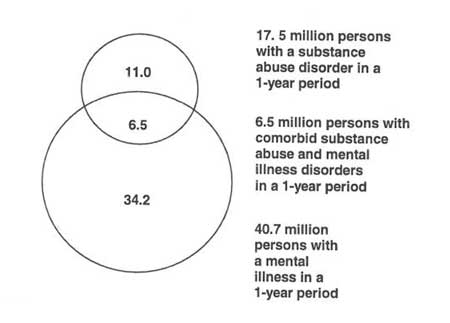 Figure 4.5 One-Year Prevalence of Alcohol and Drug Abuse and Mental Illness Among U.S. Adults Source: Narrow et al. (1993). Note: Data are extrapolations based on a nonrepresentative sample.
Figure 4.5 One-Year Prevalence of Alcohol and Drug Abuse and Mental Illness Among U.S. Adults Source: Narrow et al. (1993). Note: Data are extrapolations based on a nonrepresentative sample.Many alcohol and drug abusers have a comorbid psychiatric disorder. The graph in figure 4.6 (below) represents ECA community and institutional data that were standardized to the U.S. population. ECA estimates suggest that 52 percent of drug abusers and 35 percent of alcohol abusers had a psychiatric disorder. Twenty-eight percent of persons with a psychiatric disorder experienced either an alcohol abuse or drug abuse disorder. ECA data on the magnitude of psychiatric comorbidity among alcohol and drug abusers have been replicated by the more recent National Comorbidity Survey data (Kessler et al. 1994) and provide a reason to continue to explore the relationships that exist among co-occurring psychiatric and alcohol and drug abuse disorders. Figure 4.6 demonstrates that 22.5 percent of the general population have had a mental disorder during their lifetime, of whom 28 percent also have had an alcohol and drug abuse problem. Of the 13.5 percent of the general population who have had an alcohol abuse disorder during their lifetime, 35 percent also had a psychiatric disorder during their lifetime. Finally, of the 6.1 percent who have had a drug abuse disorder, 52 percent had a psychiatric comorbidity during their lifetime. A significant limitation to these data, however, is that one could encounter and recover from a disorder years before another disorder occurred, with no relationship between the two. It is important, therefore, to examine the prevalence of alcohol and drug abuse and psychiatric comorbidities among current clinical populations.
 Figure 4.6 Lifetime Prevalence of Comorbid Mental and Addictive Disorders in the United States
Figure 4.6 Lifetime Prevalence of Comorbid Mental and Addictive Disorders in the United StatesSource: Regier et al. (1990).
Comorbid Problems in Treatment Settings
Studies of inpatient and outpatient psychiatric populations found that comorbid psychiatric disorders occur in 30 to 50 percent of the alcohol and drug abuse treatment population; some estimates suggest that up to 80 percent of alcohol and drug abusers in treatment have psychiatric symptoms (Kosten and Kleber 1988). Other studies show that 50 to 75 percent of general psychiatric treatment populations have alcohol or drug disorders (Miller and Gold 1991). Galanter et al. (1988) reviewed the literature on patients presenting for general psychiatric treatment who are also alcohol and drug abusers and concluded that alcohol and drug abuse plays a prominent role in leading to the admissions of a majority of patients in acute psychiatric settings.
The ECA study (Narrow et al. 1993) examined the number of persons who accessed ambulatory mental health/addictive services with a diagnosis of a mental health disorder who also had an alcohol or drug abuse disorder (see table 4.21). The values ranged from 13 to 40 percent, with most of the values between 20 and 30 percent.
Table 4.22 also illustrates the percentage of mental health and alcohol and drug abuse clients with a comorbid disorder treated in inpatient facilities (mental health or general). The proportion of alcohol and drug abusers who have a co-occurring psychiatric disorder is higher than the proportion of persons with a psychiatric disorder who also have an alcohol or drug abuse disorder. However, small cell sizes for some estimates on the right-hand side of the table (mental disorders among persons with an alcohol or drug abuse disorder) suggest caution in interpretation of these estimates and highlight the need for continued research.
Research Into Causal Connections Between Psychiatric and Alcohol and Drug Abuse Disorders
Epidemiologic research indicates that alcohol or drug abuse disorders co-occur with psychiatric disorders at a rate exceeding that predicted by chance alone, suggesting that the co-occurrence between these conditions is neither random nor coincidental. The research, however, often does not clarify the nature of the relationship between the two conditions. The literature can be divided between those who suggest that alcohol or drug abuse may cause mental illness or symptoms generally indistinguishable from mental illness, and those who suggest mental illness may motivate individuals to abuse drugs or alcohol. The latter includes "self-medication" hypotheses. The objective of this study was to articulate the causal hypotheses referred to above, review the studies that have attempted to examine these causal hypotheses, and determine the cost of comorbid psychiatric and alcohol or drug abuse disorders in mental health treatment settings.
Drug and alcohol abuse are not limited to any specific group of psychiatric disorders, though they are more common among some disorders than others. Although alcohol- and drug-abusing schizophrenic persons occupy much of the time and energy of the U.S. mental health system, affective and anxiety disorders are much more common among alcohol and drug abusers (Kosten and Kleber 1988). These affective and anxiety disorders may lead to drug or alcohol abuse through efforts at self-medication, or they may result from chronic alcohol or drug abuse and be mimicked by acute intoxication (NIDA 1991a). The two causal theories are not necessarily mutually exclusive and may each play a role in the presentation of alcohol or drug abuse and mental illness comorbidity. Importantly, other factors may predispose individuals to both disorders (e.g., childhood experiences), as identified in figure 4.7.
 Figure 4.7 Variable Relationships of Causality Among Comorbid Disorders
Figure 4.7 Variable Relationships of Causality Among Comorbid DisordersHypothesis 1: Mental illness can cause alcohol and drug abuse
One source of evidence that suggests mental illness can cause alcohol and drug abuse is age-of-onset data from the ECA study. The ECA data provided evidence from retrospective self-reports by community residents of the importance of early onset of major mental disorders, especially anxiety disorders. The data included a subgroup of 4,778 respondents, ages 18 to 30, from 18,572 household respondents.
The findings demonstrated a doubling of risk for subsequent alcohol or drug abuse disorders in young adults who had an earlier depressive or anxiety disorder (see table 4.23). Similar findings are found in the work of Deykin et al. (1987), who concluded that the onset of a major depressive disorder almost always preceded alcohol or drug abuse among a sample of 424 college students ages 16 to 19. These empirical observations, however, do not address the possibility that before some people meet criteria for alcohol and drug abuse disorders, they are experimenting with or using drugs and alcohol. Initiation of licit and illicit drug use begins in early adolescence in the general population (NIDA 1990).
The self-medication hypothesis is widely used to account for high comorbidity rates between alcohol or drug abuse and psychiatric disorders. The self-medication hypothesis states that people are motivated to use drugs or alcohol to relieve psychiatric problems (Khantzian 1985). Consistent reports from patients that alcohol is used primarily to relax and relieve dysphoria suggest that the goal of self-medication spans a range of psychiatric disorders (NIAAA 1993).
Table 4.24 shows research studies that have produced findings in support of the self-medication hypothesis. The self-medication hypothesis is a clinical paradigm that attempts to enable clinicians to better understand the nature of compulsive drug and alcohol use and provides a clinical construct for consideration of treatment alternatives (Khantzian 1985). Most support for this hypothesis has been based on clinical experience.
Several researchers performed studies of narcotic addicts in inner-city New York in an attempt to understand the psychological effects of opiates and how they interacted with addicts' ego, superego, narcissism, and other psychopathology (Khantzian 1985). They posited that persons use drugs adaptively to cope with overwhelming adolescent anxiety in anticipation of adult roles in the absence of adequate preparation, models, and prospects. In the early 1970's, psychiatrists and psychologists began to study addicts within community treatment settings and their private practices.
One approach to the work placed a greater emphasis on psychological and psychiatric constructs in exploring the disturbances of addicts and understanding their suffering and subsequent addiction. This literature, based on case studies and a small sample of male inner-city opiate addicts, began to make a strong argument that psychiatric disturbances motivated opiate use to address acute and chronic anxiety (Khantzian 1985). Khantzian (1985) has concluded, based on clinical observations and psychiatric diagnostic findings of drug-dependent individuals, that drug abusers are predisposed to addiction because they suffer painful affect states and related psychiatric disorders. An addict's drug of choice is believed to be the result of an interaction between the psychopharmacologic action of the drug and the dominant painful feelings they feel. Based on clinical observations and psychiatric diagnostic findings of drug-dependent individuals, Khantzian believes narcotic addicts prefer opiates because of their powerful muting action on the disorganizing and threatening affects of rage and aggression. He also states that cocaine is an appealing drug of abuse because of its ability to relieve distress associated with depression, hypomania, and hyperactivity.
McLellan and Druley (1977) conducted a study that used the self-medication hypothesis as one explanation for patient selection of drugs with similar psychophysiological effects. McLellan reported that even though drugs may not have prevented the subsequent expression of drug abusers' psychiatric disorders, the drugs may have provided some temporary relief. These patients may have required or responded preferentially to particular drug combinations because of their underlying psychiatric symptoms. Given this self-medication explanation, the use of benzodiazepines and barbiturates by patients with underlying depression is believed to be understandable. Symptoms of anxiety, melancholy, and insomnia could be temporarily ameliorated by the anxiety-reducing, mood-elevating, and sleep-inducing effects of these drugs (NIDA 1991a).
Other researchers have found supporting evidence for the self-medication argument. Milkman and Frosch (1973) tested the hypothesis that self-selection of specific drugs is related to personality style and found distinct personality styles led heroin addicts to prefer opiates and amphetamine addicts to use amphetamines. Other researchers maintained that drug users take drugs not only to assist in defending against their feelings, but also briefly to enable the experience of feelings such as oneness with loved objects, feelings that are normally prevented by the rigid defenses against aggression (Khantzian 1985).
The results of a study conducted by McLellan and Druley (1977) suggested a correlation between use of specific drugs and psychiatric diagnosis in hospitalized psychiatric patients. Abuse of amphetamines or hallucinogens was associated with a high proportion of paranoid schizophrenia diagnoses and a low incidence of depression diagnoses: Barbiturate abuse was associated with a high proportion of depression diagnoses and a low proportion of schizophrenia diagnoses. Rounsaville et al. (1982) produced outcomes that support the hypothesis that depressed addicts use opiates as an attempt at self-medication for intolerable, dysphoric feelings. Weiss et al. (1993) found that most patients reported they used drugs and alcohol in response to depressive symptoms and experienced mood elevation, regardless of their drug of choice. However, their findings neither confirm nor negate the self-medication hypothesis of alcohol and drug abuse.
Criticisms of the self-medication hypothesis have been made by Weiss et al. (1993), Bukstein et al. (1989), Dackis and Gold (1986), and Cappell and Herman (1972). Critics have asserted that the self-medication hypothesis data do not distinguish between psychiatrically induced addictive disorders and drug-induced psychopathology. The critics argue that self-medication theory is largely based on anecdotal data, collected from small numbers of patients who have been treated in psychotherapy. They conclude that much of the self-medication theory research does not produce convincing evidence that self-medication is an important dynamic in most alcohol and drug abusers.
Hypothesis 2: Alcohol and drug abuse can cause mental illness
A significant amount of rigorously conducted research exists on the role alcohol and drug abuse play in mental illness. Most of these studies acknowledge a strong relationship between alcohol or drug abuse and mental disorders, and some of these studies report outcomes that support the hypothesis that drug or alcohol abuse can cause mental illness. However, it is important to understand that this supportive research does not state that specific types of alcohol and drug abuse always cause corresponding psychiatric disorders, but rather alcohol or drug abuse can cause mental illness (see table 4.25). The research provides evidence that alcohol and drug abusers have developed mental disorders as the result of their alcohol or drug abuse problems.
The 1991 NIDA report to Congress, Drug Abuse and Drug Abuse Research, focused a chapter on dual diagnosis. This chapter reviewed the literature and discussed studies that attempted to identify the population of dual-disordered patients and to describe the relationships between their drug of choice and their psychiatric symptoms.
In the previously discussed McLellan and Druley (1977) study of the relationship between comorbid drug abuse and mental disorders, McLellan found that significant psychiatric illnesses developed in the stimulant and depressant users groups. Two explanations were suggested for the increase in psychiatric symptoms within the two groups. McLellan established for the first time that there was evidence of measurable personality alterations associated with and specific to the chronic use of particular street drugs. One hypothesis stated that prolonged abuse of a specific combination of street drugs played a direct causal role in the resulting psychiatric disorders. This hypothesis suggested that regular consumption of particular street drugs may have hastened the development of psychiatric disorders (NIDA 1991a).
Crowley et al. (1974) suggested that drug abuse plays a prominent role in leading to the admissions of a large portion of patients into acute psychiatric services. They found that more than one-third of the adults in a psychiatric hospital had drug and alcohol abuse problems. Atkinson's research of patients seen in a psychiatric emergency service found that drugs and alcohol caused psychiatric symptoms in more than one-half of the cases, with alcohol alone in 20 percent, drugs alone in 21 percent, and both together in 12 percent of the admissions (Galanter et al. 1988). The works of Crowley et al. (1974) and other researchers strongly suggested that drug abuse played a prominent role in leading to the admissions of approximately one-third of the patients receiving acute psychiatric services (Galanter et al. 1988). Miller and Gold (1991) concluded that the acute and chronic actions of alcohol and drugs can produce symptoms similar to those found in psychiatric disorders, such as depression, anxiety, personality disorders, and psychosis.
Since McLellan's early work, there has been an increase in research examining the comoribidity relationship between alcohol or drug abuse and mental illness. Numerous studies of relatively small numbers of patients that identified what could be proposed as a causal link between specific abused substances and specific mental disorders have been carefully examined in a review by Kosten and Kleber (1988). These studies posit not that alcohol or drug abuse inevitably causes mental disorders but that specific drugs may result in a tendency for the development of mental disorders. They have identified the following patterns of drug- and alcohol-induced mental disorders:
- Users of stimulants, such as cocaine, generally present with agitated states during acute intoxication.
- Use of hallucinogens (including cannabis) can be associated with psychotic symptoms.
- A psychotic disorder can be precipitated by hallucinogens.
- Depression and mania can be either induced or mimicked by the pharmacological actions of stimulant abuse.
- Panic attacks can be induced by a variety of drugs.
- Solvents and anticholinergics can cause organic brain syndromes.
Another extensive review of literature on drug- and alcohol-induced organic mental disorders was conducted by Gold et al. (1985). They noted that the exact incidence and prevalence of these disorders is not known because it is an area of medicine and psychiatry that has been virtually ignored. Many of the studies are single-case reports, and the authors discuss the need for additional research in comorbid psychiatric and alcohol or drug abuse disorders. Tentative findings from these studies include the following:
- Adverse psychiatric reactions to marijuana and tetrahydroacannabinol (THC) included panic attacks and anxiety reactions.
- Depression severe enough to require psychiatric hospitalization has been reported in marijuana and THC users, along with acute toxic psychoses.
- Chronic opiate administration is associated with high rates of major and minor depressions. Acute effects of amphetamines are dose dependent and can include severe anxiety, panic, and acute psychoses.
- Acute toxic psychiatric effects often present as psychosis, mania, or extreme paranoia among cocaine abusers.
- Lysergic acid diethylamide (LSD) use is associated with severe panic and anxiety reactions, bipolar manic disorders, schizoaffective disorders, and major depressions.
- Inhalation of volatile fumes can have the following immediate effects: euphoria, hallucinations, conduct-disordered behavior, personality changes, irritability, anxiety, panic disorder symptoms, somatic complaints, fatigue, depression, and organic brain syndromes.
- Irritability and attacks of anger, depressed mood, and decreased social interaction may be seen in patients taking benzodiazepines or drinking alcohol.
Cost
To put the above data in perspective, it may be useful to examine the direct cost of treating mental health problems caused by alcohol and drug abuse. If alcohol and drug abuse are the underlying causes of a large amount of need for mental health treatment, then a share of the cost for these services could be attributed to both alcohol and drug abuse. Correspondingly, if underlying mental illness has caused patients to abuse drugs or alcohol, then some proportion of alcohol or drug abuse treatment services could be attributed to mental illness. The two types of cost allocations may ultimately offset each other, but it is also possible that the balance tilts more in one direction than the other. This balance may have implications for how policymakers and funders view financing of mental health and alcohol and drug abuse services.
Furthermore, treatment of comorbid mental health clients may be more complicated - and costly - than treatment of noncomorbid clients. A review in the Eighth Special Report to the U.S. Congress on Alcohol and Health (NIAAA 1993) found a series of studies concluding that patients with chronic psychiatric disorders complicated by alcohol or drug abuse have more problems than persons without alcohol and drug abuse complications. These problems include higher rates of relapse and rehospitalization, more admissions to emergency rooms, poor compliance with psychosocial and pharmacological interventions, and a history of arrests.
The research reviewed above clearly suggests that alcohol and drug abuse play important roles in contributing to, causing, and exacerbating mental disorders and may well contribute to increased admissions of persons with psychiatric disorders to mental health treatment settings. ECA data were examined to identify the percentage of patients in mental health settings who have a comorbid alcohol and drug abuse problem (Narrow et al. 1993). The following assumptions are used here to estimate the proportion of mental health expenditures that can be attributed to alcohol or drug abuse.
- Based on limited anecdotal information, it is assumed that approximately 5 percent of patients in mental health treatment settings are there primarily for alcohol or drug abuse disorders.
- One-half of the remaining comorbid population is assumed to have an alcohol or drug abuse problem that led to mental health treatment.
The best single source of information concerning expenditures for mental health services is the Inventory of Mental Health Organizations, which is summarized by the Center for Mental Health Services (Manderscheid and Sonnenschein 1994). Unfortunately, this source does not differentiate between outpatient and inpatient revenues for various types of providers (e.g., general hospitals). Accordingly, this study averages the estimated prevalence of alcohol and drug abuse disorders in psychiatric settings and applies the above-stated assumptions to derive a proportion of expenditures attributable to alcohol and drug abuse. In some cases, there was not a direct match between the ECA and Inventory of Mental Health Organization categories. For example, outpatient services from State and county mental hospitals were considered to be similar in attribution to private psychiatric hospitals. For "all other organizations," a simple average was calculated across all other settings and the same procedure used to infer attribution (subtract 5 percent and divide by 2).
These calculations suggest that as much as $3.06 billion in specialty-setting mental health treatment may have been delivered to patients seeking mental health treatment for a mental health disorder that was caused by an alcohol or drug abuse problem. This is about 9.5 percent of total mental health expenditures for the United States in 1992 (see table 4.26).
Allocations of these expenditures to drug and alcohol abuse, respectively, were based on the relative share of alcohol versus drug abusers with comorbid psychiatric disorders in the general population (refer to figure 4.6 above). Altogether, ECA data found that 6.3 percent of the population had a psychiatric disorder as well as an alcohol or drug disorder. Of these, 3.1 percent had a psychiatric disorder combined with an alcohol disorder (but not drugs), and 1.5 percent had a psychiatric disorder with a drug disorder (but not alcohol). The additional 1.7 percent had a psychiatric disorder as well as both alcohol and drug abuse disorders. This group was divided in proportion to the two prior values. It was estimated that 62.7 percent had an alcohol abuse-caused psychiatric disorder and 37.3 percent had a drug abuse-caused psychiatric disorder. Therefore, of the $3.06 billion, $1.92 billion was spent on mental health disorders attributed to alcohol abuse and $1.14 billion on mental health disorders attributed to drug abuse.
Conclusion
Preliminary - and only indicative - estimates suggest that the cost of treating alcohol- and drug- induced mental disorders may be on the order of $3.1 billion, of which 62.7 percent, or $1.9 billion, is allocated to alcohol abuse and 37.3 percent, or $1.1 billion, is allocated to drug abuse. Because of the limited amount of study and evidence on the issue, we have elected to calculate, but not to total, these costs with other estimates of health care expenditures attributable to alcohol and drug abuse. It is hoped that this analysis will stimulate more research into this issue - an issue that probably has greater clinical importance than economic impact.
It is not necessary to assume that alcohol or drug abuse, or use, began before any symptoms of mental illness in order to attribute causal involvement in an episode of treatment for mental illness. Rather, alcohol or drug abuse may exacerbate (or temporarily obscure) symptoms of mental illness. Alcohol or drug abuse may well lead to admissions to mental health treatment.
Very little is known about the etiology of alcohol and drug abuse and psychiatric problems at the subclinical level. At the extreme, the common practice of drinking a few beers to alleviate stress at the office or in the home may start a process of negative coping behaviors that culminates when a person experiences serious problems. Much more must be learned about the gateways to chronic or severe alcohol and drug abuse and the pathways to mental illness.
Medical Consequences of Violent Crime
This study estimates that $505 million in medical expenses were incurred by victims of drug- or alcohol-induced violent crime in 1992, of which $400 million was related to alcohol-induced violence and $105 million was related to drug-induced or drug-related crime. Typically, violent crimes that require medical attention include injuries and traumas, such as beatings, fractures, stab wounds, and gun shots. This study already estimates that 10 percent of all such traumas treated at hospitals or on an outpatient basis are attributable to alcohol; thus, only the $105 million attributable to drug abuse is added separately. A full discussion of alcohol and drug abuse-related crime, including violent crime, is included in chapter 6, and the assumptions underlying this calculation are shown in appendix C, table 7.
- Table 4.17: Total Monthly Cost of Treating Person With HIV by Disease Stage
-
Table 4.17: Total Monthly Cost of Treating Person With HIV by Disease Stage (1992 dollars) Type of Care Phase 1
HIV Positive Without AIDS
(T-Cell Count >= 0.5 x 109/L)Phase 2
HIV Positive Without AIDS
(T-Cell Count >= 0.2 x 109L and < 0.5 x 109/L)Phase 3
HIV Positive Without AIDS
(T-Cell Count < 0.2 x 109/L)Phase 4
Persons With AIDSInpatient $54 $119 $456 $1,890 Outpatient visits $151 $191 $344 $380 Home health $10 $21 $80 $174 Drug costs $67 $99 $110 $265 Long-term care $0 $0 $0 $55 Total Costs $282 $430 990 $2,764 Source: Hellinger (1993).
Note: Components may not sum to totals because of rounding.
- Table 4.18: Total Lifetime Cost of Treatment for HIV Infection From Onset to Death
-
Table 4.18: Total Lifetime Cost of Treatment for HIV Infection From Onset to Death (1992 dollars) Disease Stage Mean Duration of Phase (months) Cost per Month Total Cost of Care HIV positive without AIDS (phase 1) (T-cell >= 0.5 x 109/L) 67.3 $282 $18,978 HIV positive without AIDS (phase 2) (T-cell count >= 0.2 and < 0.5 x 109/L) 44.0 $430 $18,920 HIV positive without AIDS (phase 3) (T-cell count < 0.2 x 109/L) 12.4 $990 $12,276 Person with AIDS (phase 4) 25.0 $2,764 $69,100 Course of Illness 148.7 $4,466 $119,274 Source: Derived from Hellinger (1993).
Note: Components may not sum to totals because of rounding.
- Table 4.19: Treatment Costs per Acute Hepatitis B Virus Case
-
Table 4.19: Treatment Costs per Acute Hepatitis B Virus Case Disease Stages/Conditions Probability of Stage
(%)Number of Cases in 1992 Cost per Case in 1992 Total HBV Treatment Expenditures
(millions of dollars)Total IVDU-Related HBV Expenditures
(millions of dollars)Acute Disease Only Subclinical 65.7 131,400 $6 $0.8 $0.1 Clinical, nonfulminant 34.0 68,000 $703 $47.8 $5.7 Fulminant 0.3 600 $12,124 $7.2 $0.9 Subtotal, Acute 100.0 200,000 NA $55.9 $6.7 Chronic Disease Chronic carrier state 3.9 2,657 $950 $2.5 $0.3 Chronic persistent state 2.0 1,363 $1,618 2.2 $0.3 Chronic active hepatitis 2.6 1,771 $67,486 $119.6 $14.3 Primary hepatic cancer 1.3 886 $103,148 $91.4 $11.0 Subtotal, Chronic 6-10 6,677 NA $215.6 $25.9 Total, All Conditions $271.5 $32.6 Source: Bloom et al. (1993).
Note: Components may not sum to totals because of rounding. Intravenous drug use is estimated to cause 12 percent of hepatitis B (HBV) cases.
- Table 4.20: Treatment Costs per Acute Hepatitis C Virus Case
-
Table 4.20: Treatment Costs per Acute Hepatitis C Virus Case Disease Stages/Conditions Probability of Stage
(%)Number of Cases in 1992 Cost per Case in 1992 Total HCV Treatment Expenditures
(millions of dollars)Total IVDU-Related HCV Expenditures
(millions of dollars)Acute Disease Only Subclinical 65.7 111,690 $6 $0.7 $0.3 Clinical, nonfulminant 34.0 57,800 $703 $40.6 $14.6 Fulminant 0.3 510 $12,124 $6.2 $2.2 Subtotal, Acute 100.0 170,000 NA $47.5 $17.1 Chronic Disease Chronic carrier state 24.9 14,420 $950 $13.7 $4.9 Chronic persistent state 12.5 7,239 $1,618 $11.7 $4.2 Chronic active hepatitis 16.3 9,440 $67,486 $637.1 $229.3 Primary hepatic cancer 8.1 4,691 $103,148 $483.9 $174.2 Subtotal, Chronic ˜50 35,790 NA $1,146.3 $412.7 Total, All Conditions $1,193.8 $429.8 Source: Bloom et al. (1993).
Notes: Components may not sum to totals because of rounding. Intravenous drug use is estimated to cause 36 percent of hepatitis C (HCV) cases. Total probability of chronic disease stage (50 percent) is less than the sum of specific categories because more than one category of chronic stage is possible with any given case.
- Table 4.21: Ambulatory Mental Health Patients With Alcohol or Drug Abuse Disorder
-
Table 4.21: Ambulatory Mental Health Patients With Alcohol or Drug Abuse Disorder Ambulatory Mental Health Settings Percent
(N= 1,904)Psychiatric hospital outpatient clinic 25.2 Mental health center outpatient clinic 18.4 General hospital outpatient clinic 19.0 VA hospital outpatient clinic 40.6 Alcohol/drug unit outpatient clinic 35.0 Mental health specialist in health plan/clinic 17.7 Mental health specialist in private practice 16.1 Crisis center 28.0 Emergency department 41.9 General medical physician 15.2 Family/social service agency 14.6 Clergy/religious counselor 13.5 Natural therapist 29.1 Other human services 23.6 Self-help group 33.2 Friend/relative 15.4 Source: Narrow et al. (1993).
Note: VA = Veterans Affairs.
- Table 4.22: Comorbidity Among Inpatient/Residential Patients Treated in Specialty Mental Health/Alcohol and Drug Abuse Settings
-
Table 4.22: Comorbidity Among Inpatient/Residential Patients Treated in Specialty Mental Health/Alcohol and Drug Abuse Settings Inpatient Setting Persons With a Mental Disorder Who Also Have an Alcohol and Drug Abuse Disorder (%) Persons With an Alcohol and Drug Abuse Disorder Who Also Have a Mental Disorder (%) General hospital (psychiatric unit and scatter-bed) 39.3 72.9 State and county mental hospitals 22.1 95.0 Residential supportive care 27.7 98.6 Community mental health center 1.2 81.0 Private mental hospital 19.3 77.7 VA hospital psychiatric unit 77.7 82.1 Alcohol/drug treatment unit 56.8 97.4 Nursing home 15.6 100.0 Source: Analysis of Narrow et al. (1993) by The Lewin Group.
Note: VA = Veterans Affairs.
- Table 4.23: Prevalence and Age at Onset of Alcohol Abuse, Drug Abuse, Major Depression, and Anxiety in the Epidemiologic Catchment Area Study
-
Table 4.23: Prevalence and Age at Onset of Alcohol Abuse, Drug Abuse, Major Depression, and Anxiety in the Epidemiologic Catchment Area Study Disorder (Lifetime Diagnosis) Prevalence
(%)Mean Age at Onset
(years)Alcohol abuse or dependence 13.3 23.2 Drug abuse or dependence 5.9 20.2 Major depressive episode with mania 0.5 19.3 Anxiety disorders 14.6 19.6 Source: Christie et al. (1988).
- Table 4.24: Studies on Mental Disorder-Induced Drug and Alcohol Abuse
-
Table 4.24: Studies on Mental Disorder-Induced Drug and Alcohol Abuse Mental Illness Disorder Relationship Substance Citation Major depressive Associated Alcohol, drugs Deykin et al. 1987 Social phobia Associated Alcohol Judd 1994 Traumatic neurosis Self-medication Alcohol Lacoursiere et al. 1980 Major depressive episode and anxiety Associated Drugs Christie et al. 1988 Depression Associated Cocaine Kosten et al. 1987 Depression, hypomania, and hyperactivity Self-medication/ self-selection Cocaine Khantzian 1985 Altered ego state Associated/ self-selection Heroin Milkman and Frosch 1973 Rage and aggression Self-medication/ self-selection Heroin Khantzian 1985 Depression Supports self-medication Opiates Rounsaville et al. 1982 Premorbid adaptation Self-selection Amphetamines Milkman and Frosch 1973
- Table 4.25: Studies on Drug and Alcohol Abuse-Induced Mental Illness
-
Table 4.25: Studies on Drug and Alcohol Abuse-Induced Mental Illness Drug Substance Relationship Mental Illness Disorder Citation Cocaine and amphetamine Associated Bulimia nervosa and anorexia nervosa Hudson et al. 1992. Cocaine and marijuana Associated Obsessive-compulsive disorder Crum and Anthony 1993 Cocaine Associated Panic attacks Rosen and Kosten 1992 Cocaine Associated Panic disorder Louie et al. 1989 Cocaine and phencyclidine (PCP) Can cause Panic disorder Price and Giannini 1987 Cocaine Can cause Panic disorder Aronson and Craig 1986 Opiates Associated Major and minor depression Croughan et al. 1982 Alcohol Induce Depression and temporary organic brain syndrome Schuckit 1983 Alcohol Associated Depression Powell et al. 1982 Alcohol Associated Depression Schuckit 1986 Alcohol and drugs Can produce Depression, anxiety, psychoses, and personality disorders Miller and Gold 1991 Phencyclidine (PCP) Associated Acute psychiatric exacerbations Yago et al. 1981
- Table 4.26: Costs of Mental Health Services Provided to Persons With an Alcohol- or Drug-Induced Mental Illness, 1992
-
Table 4.26: Costs of Mental Health Services Provided to Persons With an Alcohol- or Drug-Induced Mental Illness, 1992 (millions of dollars) Type of Organization Total Expenditures Cases Attributed to Alcohol and Drug Disorders (%) Cost Attributed to Alcohol or Drug Abuse State and county mental hospitals $8,797 9.3% $820 Private psychiatric hospitals $6,904 8.6% $595 Non-Federal general hospitals with psychiatric services $5,275 12.1% $637 VA medical centers $1,675 10.7% $179 Residential treatment centers for emotionally disturbed children $2,228 7.2% $159 Freestanding psychiatric outpatient clinics $759 6.7% $51 All other organizations $6,510 9.5% $620 Total $32,148 $3,062 Sources: Narrow et al. (1993); Manderscheid and Sonnenschein (1994).
Note: Components may not sum to totals because of rounding.