Purpose of This Report
Alcohol and drug abuse impose a variety of costs on our society. The aim of this study is to quantify the adverse outcomes of alcohol and drug abuse and express the magnitude of these consequences using the common metric of money. It is hoped that this information will contribute to a better understanding of the nature and magnitude of the impact of alcohol and drug abuse and that this understanding will help decisionmakers to identify appropriate strategies to reduce these adverse effects.
Economic analyses of alcohol and drug abuse disorders provide a convenient means of quantifying the effects of alcohol and drug abuse, effectively stating these impacts in "dollars." It is abundantly clear, however, that there are effects of alcohol and drug abuse for which no economic analysis method or data base has yet been developed, and so this economic analysis cannot be complete.
The work represented in this report builds on a strong history of cost-of-illness studies conducted for more than 40 years. This report relies on the methods adopted by the U.S. Public Health Service, which were implemented in previous cost-of-illness studies of alcohol and drug abuse and mental health (Cruze et al. 1981; Harwood et al. 1984; Rice et al. 1990).
This report estimates the economic impact of alcohol and drug abuse for 1992. The year 1992 was selected as the most recent for which a wide variety of data were available at the time this study was undertaken. The most recent estimation by Rice and her colleagues was reported for 1990, but it relied mainly on inflation-adjusted data collected from 1985 (Rice 1993). Important changes in the organization and nature of health services, employment, and crime have taken place during the period between the last cost-of-illness study and 1992, necessitating a reexamination of costs with more up-to-date data. Section 2.2 describes the extent of the alcohol and drug abuse problems in 1992 and provides more background on the history and role of cost-of-illness studies.
This report is designed to serve as a tool for policy analysts and researchers with questions about the consequences and costs associated with alcohol and drug abuse. However, caution is urged that the data included in this report not be overinterpreted. For example, it is essential to point out that "high costs" do not necessarily translate into high marginal benefit from public policy changes. The data contained in this report are not an evaluation of the efficacy or impact of interventions; rather, these data may serve as a baseline to be used to understand or interpret potential changes.
Background
Alcohol and Drug Abuse and Dependence in 1992
The use of alcohol, tobacco, and illicit drugs, such as cocaine and heroin, account for many preventable health conditions and other problems common in the United States. However, alcohol or drug use does not equate to alcohol or drug abuse. In fact, alcohol and drug use ranges in severity from casual use to moderate use, alcohol and drug abuse, and alcohol and drug dependence - each potentially manifesting different types of consequences. The American Psychiatric Association (1994) has provided the following definitions of abuse and dependence:
- Alcohol or drug abuse is a maladaptive pattern of alcohol or drug use manifested by recurrent and significant adverse consequences related to the repeated use of alcohol or drugs.
- Alcohol or drug dependence involves a cluster of cognitive, behavioral, and physiological symptoms that result from repeated self-administration that usually results in tolerance, withdrawal, and compulsive drug-taking behavior.
Based on a household survey of 42,862 adults conducted in 1992, the National Longitudinal Alcohol Epidemiologic Survey (NLAES) (Grant and Dawson 1996) provides nationally representative estimates of alcohol and drug abuse as well as dependence. Based on use patterns and symptoms in the past year (1992), NLAES data indicate the following:
- 7.4 percent of the U.S. adult population - more than one-half of the Nation's heavy drinkers - were dependent on (4.4 percent ) or abusers of (3.0 percent) alcohol, and
- 1.5 percent of the U.S. adult population (about 30 percent of the Nation's drug users) were dependent on (0.5 percent) or abusers (1 percent) of drugs.
Analyses of NLAES have also concluded that the younger the age of onset of drinking, the greater the chance that a person will develop a clinically defined alcohol disorder (National Institute on Alcohol Abuse and Alcoholism 1998). Youth who began drinking before they turned 15 were twice as likely to develop an alcohol abuse problem and four times more likely to develop alcohol dependence, compared with persons who did not begin drinking before age 21. More than 40 percent of respondents who began drinking before age 15 were classified as alcohol dependent at some time in their lives.
National statistics on the prevalence of alcohol and drug abuse only echo the personal experience of family members, friends, employers, and others who daily come into contact with alcohol- and drug-dependent persons. It is important to remember that many alcohol and drug users, even regular users, may continue for extended periods of time to lead functional, relatively balanced, and productive lives.
Trends in Alcohol and Drug Use Before and Since 1992
Even limited consumption of mind-altering substances may result in drastic consequences: Motor vehicle crashes that occur when intoxicated persons drive and overdoses of drugs or alcohol are a few examples. Though some types of economic impact may only result from long-term heavy consumption that is frequently associated with dependence (e.g., the costs of treating liver cirrhosis), any abuse of alcohol or drugs has the potential to impose costs on society.
Analysis of the 1992 National Household Survey on Drug Abuse (NHSDA) (Substance Abuse and Mental Health Services Administration 1995) indicates that in 1992 more than 1 in 10 civilians, noninstitutionalized U.S. residents over the age of 12 used illicit drugs, and about two-thirds of this same population drank alcohol. It is estimated that there were 47.8 million current drinkers (defined as those who drank within the past month) and 11.4 million current illicit drug users. Additional alcohol and drug use is found among noncivilians, institutionalized persons (e.g., prisoners), and children younger than 12.
During 1992, NHSDA data indicate that approximately 133 million persons drank alcohol and 22.9 million persons consumed illicit drugs during the previous year. Marijuana and hashish, the most commonly used illicit drugs, were used by 17.4 million persons in 1992. Psychotherapeutic drugs, such as stimulants, sedatives, tranquilizers, and analgesics, were used for nonmedical reasons by 7.8 million persons; cocaine in all forms, including crack, was used by almost 5 million persons. Inhalants and hallucinogens were used by 2.0 and 2.4 million persons, respectively. Although the design of the NHSDA may underestimate alcohol and drug abuse among certain populations, data suggest that more than 800,000 persons used cocaine and more than 320,000 persons used heroin - both of which receive considerable media attention.
Estimates of alcohol and drug use for 1992 show a continuing decline that began during the late 1970's or early 1980's (see figure 2.1 and figure 2.2 below). Data from the NHDSA show declines in "current" alcohol and drug use (measured as consumption in the prior month) until 1992, including the following:
- A drop in alcohol use from 76 percent in 1979 to 59 percent in 1992 among 18- to 25-year-olds and from 61 percent in 1979 to 50 percent in 1992 among adults over age 25;
- A drop in marijuana and hashish use from 35 percent in 1979 to 11 percent in 1992 among 18- to 25-year-olds and from more than 6 percent in 1982 to 3 percent in 1992 among adults over age 25; and
- A drop in cocaine use (including crack cocaine) from 9 percent in 1979 to under 2 percent in 1992 among 18- to 25-year-olds, and from 2 percent in 1985 to 0.5 percent in 1992 among adults over age 25.
However, alcohol and drug use has increased modestly since 1992. Particularly troubling are dramatic increases in drinking and illicit drug use - including use of marijuana, cocaine, and inhalants - among the Nation's 12- to 17-year-olds. Nearly twice as many adolescents took drugs in the month before being interviewed in 1995 than was the case 2 years before. Heroin use among young adults increased before 1992, rising from 0.3 percent among 18- to 25-year-olds in 1988 to 1.3 percent in 1992.
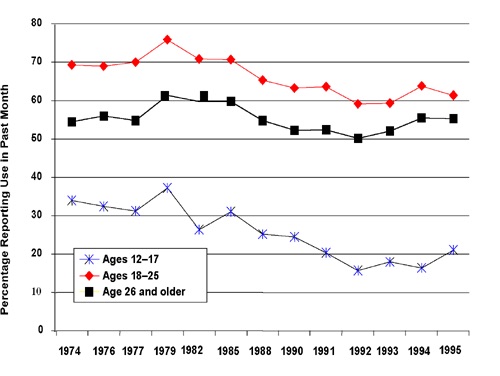 Figure 2.1 Estimated Prevalence of Alcohol Use in the Past Month, 1974 -1995 Substance Abuse and Mental Health Services Administration. Office of Applied Studies. National Household Survey on Drug Abuse: Main Findings and Population Estimates (multiple years, 1992-1996).
Figure 2.1 Estimated Prevalence of Alcohol Use in the Past Month, 1974 -1995 Substance Abuse and Mental Health Services Administration. Office of Applied Studies. National Household Survey on Drug Abuse: Main Findings and Population Estimates (multiple years, 1992-1996).Illicit drug use was more common among males, residents of large metropolitan areas, college students, and unemployed persons than among other demographic groups in 1992. Males were about 1.5 times as likely to have used illicit drugs in the past year as females (13.4 percent versus 9.0 percent). About 12.1 percent of residents in large metropolitan areas used illicit drugs in the past year, compared with 10.4 and 10.3 percent of residents in smaller metropolitan and nonmetropolitan areas. About 13.7 percent of persons who went to college but did not graduate used illicit drugs in the previous year (compared with 9.8 percent of high school noncompleters, 11.5 percent of high school graduates, and 8.9 percent of college graduates). Finally, and most significantly, 24.0 percent of unemployed persons (excluding 12- to 17-year-olds) consumed illicit drugs versus 12 to 14 percent of employed persons and 5.8 percent of persons not in the labor force.
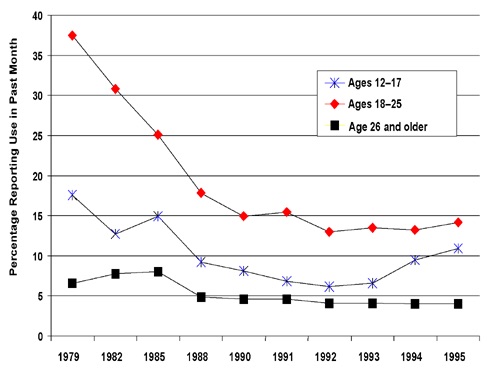 Figure 2.2 Estimated Prevalence of Any Illicit Drug Use in the Past Month 1974-1995 Substance Abuse and Mental Health Services Administration. Office of Applied Studies. National Household Survey on Drug Abuse: Main Findings and Population Estimates (multiple years, 1992-1996). Note: Estimates with low precision or years with no estimates reported are excluded
Figure 2.2 Estimated Prevalence of Any Illicit Drug Use in the Past Month 1974-1995 Substance Abuse and Mental Health Services Administration. Office of Applied Studies. National Household Survey on Drug Abuse: Main Findings and Population Estimates (multiple years, 1992-1996). Note: Estimates with low precision or years with no estimates reported are excludedIn contrast to data from the NHSDA, which are more likely to capture casual use, data from the Drug Abuse Warning Network (DAWN) reflect more intense use. Although casual use has declined dramatically since the late 1970's, indicators of intensive use have significantly increased since that time. According to 1993 DAWN data, an estimated 466,900 drug abuse-related emergency room episodes occurred in the United States. This is a 16-percent increase from 403,600 in 1988 (U.S. Department of Health and Human Services 1994c). The rate of drug-related episodes per 100,000 persons age 6 and older increased from 186 in 1988 to 204 in 1993.
The Need To Reestimate Costs
Numerous studies of the economic impact of alcohol and drug abuse problems have been reported on over the past 30 years. Three comprehensive studies were completed within the past 15 years, including two studies conducted by Research Triangle Institute (Cruze et al. 1981; Harwood et al. 1984) and one by the Institute for Health and Aging, University of California, San Francisco (Rice et al. 1990). The Rice et al. study (1990), the most recent estimate available, reported economic costs based on 1985 data. Rice et al. (1990) found that alcohol and drugs together cost the United States more than $114 billion in 1985, more than one-half of which was due to lost productivity resulting either from premature mortality or from other factors associated with alcohol and drug abuse. Rice (1993) projected the 1985 alcohol estimates forward to 1990, primarily adjusting for inflation but relying on the same data collected during 1985. Similar summary projections of the drug abuse estimates to 1990 were reported in a Robert Wood Johnson Foundation report (Institute for Health Policy 1993).
Important changes have taken place in the past decade, underscoring the need to reestimate the costs of alcohol and drug abuse using up-to-date information. Among these changes are the following:
- Changes in the prevalence of alcohol and drug use disorders;
- Rapid spread of HIV and its primary sequela, AIDS, among intravenous drug users;
- Increased availability of cocaine and crack cocaine;
- Increases in crime and violent crime, which are possibly related to the drug trade;
- Passage of stricter drunk driving laws; and
- Increased availability of, and support for, alcohol and drug abuse treatment (largely during the late 1980's).
Alcohol and drug use disorders carry with them several wide-ranging and well-recognized sequelae, including the following:
- Health outcomes of alcohol and drug abuse problems and their subsequent impact on the health care system;
- Job loss, financial destitution, and reliance on society's safety nets; and
- Criminal behavior, including income-generating crimes, participation in the drug trade, and violence.
This report relies on an extensive array of data sources, including secondary analyses of nationally representative data bases, where available; literature reviews; and contacts with topical experts. Different topical areas are more or less "data rich." In particular, estimating the causal roles played by alcohol and drug abuse presents a challenge to the analyst. This report generally aimed to remain "conservative" when reaching conclusions, especially for cases where some amount of judgment was required; however, in some instances, less conservative estimates were supported by the research. For example, if a range of estimates of causality were available, researchers for this study picked a midrange value if it was defensible, but in some cases, they chose a value at the low end of the range. With this or any large study that presents the research evidence available at a moment in time, it is possible that newer research findings eventually may supplant some evidence reported. One important finding of this report, in fact, is that much more data and analyses of the specific roles played by alcohol and drug abuse in a variety of related problem areas are needed.
Scope of This Study
This study estimates the economic value of many consequences associated with the abuse of alcohol, illicit drugs, and other drugs taken for nonmedical purposes. Types of consequences include health problems and health care utilization, effects on productivity, and other costs, including crime and social welfare. This study did not collect primary data, but rather conducted analyses of secondary data sources. A thorough discussion of analytic principles used in estimating the cost of alcohol and drug abuse is provided in chapter 3. In general, this report identifies and estimates the economic value of adverse outcomes stemming from the misuse, abuse, and dependence on alcohol and drugs. Moreover, this report relies primarily on estimates of the value of goods and services and lost productivity stemming from alcohol and drug problems. Other effects or costs that one might expect to occur as a result of alcohol and drug abuse (e.g., pain and suffering) are not estimated here chiefly because of the lack of reliable and complete data.
Certain analyses of the economic costs of alcohol and drug abuse are included here, while other analyses might be undertaken at a later date. This study estimates the relative burden borne by government, employers, families, and others. It is infeasible in this comprehensive study, however, to fully consider the effects of the following on any or all of the consequences of alcohol and drug abuse:
- The roles of particular illegal drugs (e.g., heroin, cocaine, and marijuana) and particular categories of alcoholic beverages (e.g., beer, wine, and distilled spirits) separately or in combination with other substances;
- The effects of different modes of drug consumption (e.g., injection, smoking/inhalation, and oral); or
- The implications of different potencies for any of the substances under consideration.
There may be reasons to undertake a cost study of a particular substance, mode of consumption, or potency of substance. Public policy may be informed by such analyses. For example, such analyses could help to inform debates regarding (1) legal sanctions against drugs such as marijuana, powder cocaine, or crack cocaine; (2) taxation on smokable versus oral tobacco products; and (3) differential regulation of beer, wine, and distilled spirits. In theory, such analyses should be possible, although it may be difficult in practice because of data limitations.
Because many alcohol or drug abusers use multiple psychoactive substances (particularly illicit substances), developing estimates of the costs of particular substances can be difficult. Good epidemiological and etiological research should attempt to address this issue. However, the drugs and their patterns of use change continuously and rapidly, making it difficult to define and study consequences and costs associated with single substances.
Extensions of the analysis reported here could focus on particular patterns or situations of use. Two examples of this are the hypotheses that (1) consumption of high levels of alcohol poses greater risks when it occurs outside rather than inside the home, and (2) injection of drugs presents different risks than smoking and inhalation.
Future cost-of-illness studies might also consider the health benefits (primarily cardiovascular) associated with moderate consumption of alcoholic beverages. Those health benefits are acknowledged but not addressed in this report. This is indeed an important avenue for future research, and it does add a new dimension to our understanding of the economic impact of alcohol consumption in our Nation. However, this study estimates only the negative impact of drug and alcohol abuse and dependence. Its intent has not been to compare the negative effects with the benefits of alcoholic beverages (or psychoactive drugs). While a cost-of-illness study chronicles the damage of improper use and behaviors - which society properly strives to reduce - it does not constitute a summary judgment of the social or economic value of psychoactive alcohol and drugs in society.
The contributions of the alcoholic beverage industry to the U.S. economy are substantial, and alcoholic beverages are consumed safely by most consumers. In addition, there is credible evidence that moderate consumption of alcoholic beverages may have a positive impact on cardiovascular health. The nearly $75 billion that consumer surveys estimate is spent on alcoholic beverages per year (U.S. Department of Commerce 1993) is a meaningful part of the benefits perceived by consumers from consumption of these products. However, it is not correct - in fact, it is meaningless - to compare expenditures with negative economic effects and make summary judgments about how society should view and address alcoholic beverages. The proper level of analysis would be to examine specific public policies regarding alcohol consumption and to analyze their benefits and costs. This study yields data that could be useful in designing and performing such analyses, but it produces few insights into the justification for particular alcohol control policies.
Similarly, the results of this study yield few insights into specific policies to control drug abuse or into the alternatives of drug prohibition versus legalization. The purpose of this study has been to identify and quantify particular negative consequences from the abuse of and dependence on alcohol and illicit drugs. Such data may - and indeed should - inform the evaluation of particular policies. However, this study has not attempted such an undertaking.
Overview of the Report
Following the guidance for cost-of-illness studies adopted by the U.S. Public Health Service (Hodgson and Meiners 1979, 1982), this report is organized to differentiate health costs from non-health costs and the value of goods and services from the value of lost productive potential. The remaining chapters of this report are organized as follows:
- Chapter 3 describes the analytic principles underlying cost-of-illness studies such as this, including the history of these studies in alcohol and drug abuse. The chapter also describes the framework for estimating the consequences, causal role, and associated costs of alcohol and drug abuse.
- Chapter 4 discusses the health costs directly attributed to alcohol and drug abuse, including specialty alcohol and drug abuse treatment, and treatment for health conditions caused by alcohol or drug abuse.
- Chapter 5 presents the estimates of productivity losses due to alcohol and drug abuse associated with premature deaths; foregone productivity in the workplace and the home; and lost productivity due to institutionalization, incarceration, victimization, and participation in criminal enterprises.
- Chapter 6 presents the costs of crime and criminal justice system expenditures, the costs of motor vehicle crashes, and social welfare costs that result from alcohol and drug abuse, as well as lost legitimate earnings among people in society who are affected by, but not necessarily directly engaged in, alcohol or drug abuse.
- Chapter 7 concludes this study by answering the questions, "Who bears the costs of alcohol and drug abuse?" and "How do the results of this study compare to previous estimates of alcohol and drug abuse costs?" Additional priorities for research are also identified in chapter 7. Supporting materials and detailed tables are included in the appendixes.
This report is organized into discrete sections within each chapter so that the reader does not have to read the entire report in order to understand a particular issue or topic of interest. For example, a discussion of the cost of fetal alcohol syndrome in 1992 is fully contained in chapter 4, section 4.4.1. Each section discusses the prevalence or the magnitude of problems potentially related to alcohol and drug abuse, estimates of the amount of the problems caused by alcohol and drug abuse, and estimates of the costs associated with the problem. Some of the consequences of alcohol and drug abuse, however, result in health care, productivity, and other costs. Such is the case with alcohol-related motor vehicle crashes or alcohol- and drug-related crime, which contribute to costs reported in chapters 4, 5, and 6.