 Dr. Marco Diana
Dr. Marco Diana Dr. Diana Martinez
Dr. Diana MartinezIn Part 1:
A few years ago Dr. Diana Martinez and Dr. Marco Diana decided to investigate a new technology that uses magnetic pulses to stimulate brain cells. Both had been trying to develop medications to treat cocaine addiction, and both had come to feel that the pace of progress—their own and others'—was unequal to the urgency of the need. In the new technology, transcranial brain stimulation (TMS), they saw a potential treatment that might be developed relatively rapidly for clinical use.
Dr. Martinez, a neuroimaging specialist at Columbia University Health Center in New York City, planned a preclinical study. She was using a relatively new type of TMS coil (magnetic pulse generator), and her first objective was to identify machine settings with potential clinical efficacy.
Participants in her study were cocaine users who did not want to stop. They came into the hospital research unit, and attended a self-administration session in which they repeatedly chose between smoking a dose of the drug and receiving a sum of money. They then underwent TMS for 3 weeks, after which they repeated the self-administration session. If they chose cocaine less often after treatment than they had before, the setting that was used would be a good candidate for further testing.
Dr. Diana, a research pharmacologist at the University of Sassari, Italy, designed a pilot clinical trial. Sixty people who were trying to quit cocaine would receive TMS, real or sham, every other day for a month. Dr. Diana would assess their cocaine use though interviews and hair analysis before they started TMS, at the end of the treatment month, and every 3 months thereafter for a year. He hoped that the patients who received real TMS would reduce their cocaine use.
Both researchers' projects hit snags early on. In this installment, we follow Dr. Martinez as she resolves an initial impasse and advances her project to a new stage. Meanwhile, circumstances close in on Dr. Diana. He is forced to cut short his trial, but comes away with encouraging data and increased enthusiasm for TMS.
Frequency and Intensity
The first TMS settings Dr. Martinez tested appeared to reduce cocaine intake among participants who completed the course of treatment. However, only one third completed the course. The rest complained of pain and anxiety during their first treatment session, and refused to continue.
Dr. Martinez adjusted one of her settings to try to prevent patient dropout. Reducing the magnetic pulse frequency from 10 Hz to 1 Hz abolished the aversive responses, but also the reductions in cocaine use.
Dr. Martinez considered testing an intermediate frequency. In the end, she decided to look for a way to make 10 Hz more tolerable. She says, "If you look at the literature on TMS in psychiatric disorders, there’s a strong rationale for using 10 Hz, or even 15 or 20 Hz."
She asked herself why so many participants hadn’t tolerated TMS at 10 Hz, when many other researchers had used it without problems. Of several possible explanations, one stood out: Cocaine users tend to have exceptionally high motor thresholds.
Dr. Martinez explains, "A person's motor threshold is the lowest TMS intensity that will stimulate his or her motor neurons to fire and contract a muscle. The TMS technician ascertains the motor threshold to determine how much stimulus to apply in treatment. If the stimulus is strong enough to activate motor neurons, it’s presumably enough to activate neurons in other cortical areas as well."
To ascertain the motor threshold, the technician directs the TMS pulse at an area of motor cortex that controls a muscle, for example a hand or calf muscle. The technician delivers a pulse at a low intensity setting, then dials the intensity up in small steps until the target muscle twitches. The twitch gives visible proof that motor neurons have fired.
Dr. Martinez says, "The motor thresholds of the cocaine users in our study were in the range of 80 percent to 84 percent of the power output of our TMS coil. That's higher than the thresholds that have been recorded in other studies with coils of this type. It's also been reported in the literature that cocaine users have high motor thresholds."
Because of their high motor thresholds, Dr. Martinez’ study participants received exceptional amounts of stimulation during the ascertainment procedure. She says, "We had to keep turning up the intensity of the stimulus, and it would often take us a good 40 minutes to work up to the threshold." Maybe, she thought, so much stimulation during the ascertainment, plus the additional stimulation applied during treatment, hyper-excited neurons in a way that caused pain and alarm.
Dr. Martinez tested her conjecture on herself. She recounts, "When we first started working with TMS, I was curious about the experience, so I went under the coil to ascertain my motor threshold. I found out that, like cocaine users, I tend to have a higher threshold than the average person. During the ascertainment procedure I developed a headache and some other mild symptoms, but nothing too unpleasant. Now I decided to see how I would feel if I underwent what our study participants were getting—motor threshold ascertainment followed by a 10-Hz treatment. I was miserable."
Tweak and Succeed
Dr. Martinez considered how she might adjust her study protocol to make TMS at 10 Hz comfortable for cocaine users despite their high motor thresholds. She could obtain no guidance from colleagues or the scientific literature, because no one had ever before used the specific TMS coil she was using, called the H coil, with cocaine users.
Dr. Martinez turned for advice to Dr. Abraham Zangen, of Ben-Gurion University of the Negev, in Israel, a researcher and developer of the H coil. Brainstorming together, the two came up with two adjustments:
- Dr. Martinez had been administering TMS treatment directly after motor threshold ascertainment. Going forward, she would separate the two: ascertain the motor threshold in the morning and deliver treatment in the afternoon. Doing so would spread the stimulation over a longer time.
- She would lower the intensity of the TMS treatment. Dr. Zangen had been using the H coil to treat patients with obsessive compulsive disease, and had found that intensities lower than the motor threshold could be effective.
Dr. Martinez says that when she returned to the TMS laboratory, "We weren't sure that these adjustments would work. We were nervous. And the participants picked up on our unease. They were looking at us like, 'Why are you nervous?'"
The adjustments worked (see Figure). Participants no longer reported pain, and most now stayed on to complete the treatment. A further protocol adjustment—spreading motor threshold ascertainment over 4 days—further increased the completion rate.
Dr. Martinez says, "These adjustments to our protocol give people time to acclimate to the stimulation. We've seen that TMS definitely gets less painful over time."
With the amended protocol, Dr. Martinez quickly reached her goal of treating 6 participants with TMS at 10 Hz. These patients reduced their choices for cocaine, from about 5.5 before the treatment to 2.2 after it. No changes in the choice for cocaine were seen in the groups that received sham or low-frequency TMS.
Dr. Martinez says, "I must thank Dr. Zangen, who spent a lot of time discussing ways to fix my protocol. I'm also grateful to Brainsway Corporation, makers of the H coil, who have a real interest in treating addiction, and provided me with the equipment to do this work."
Judging that she had enough evidence that her TMS protocol was efficacious to warrant a pilot clinical trial, Dr. Martinez began to prepare a grant proposal. In the next installment of this Narrative of Discovery, we'll follow Dr. Martinez into this next stage of her project.
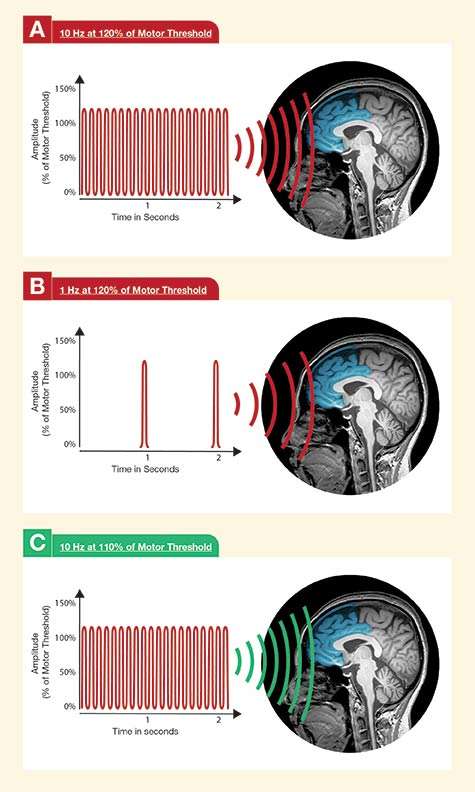 Figure. TMS Frequency and Intensity Settings Determine Efficacy and Tolerability In Dr. Martinez’ study, participants who completed a course of TMS with a frequency of 10 hertz (Hz, pulses per second) (A) reduced their cocaine use, but many found the treatment intolerable. Participants tolerated TMS with a frequency of 1 Hz well (B), but did not reduce their cocaine use. Dr. Martinez adjusted the schedule of her TMS protocol and tried 10 Hz again, this time with success. For her final settings, she also lowered the TMS pulse intensity (amplitude) from 120 percent of motor threshold to 110 percent of motor threshold (C).
Figure. TMS Frequency and Intensity Settings Determine Efficacy and Tolerability In Dr. Martinez’ study, participants who completed a course of TMS with a frequency of 10 hertz (Hz, pulses per second) (A) reduced their cocaine use, but many found the treatment intolerable. Participants tolerated TMS with a frequency of 1 Hz well (B), but did not reduce their cocaine use. Dr. Martinez adjusted the schedule of her TMS protocol and tried 10 Hz again, this time with success. For her final settings, she also lowered the TMS pulse intensity (amplitude) from 120 percent of motor threshold to 110 percent of motor threshold (C).
- Text Description of Graphic
-
The figure is arranged in three panels (A, B, and C), each showing on the left a graph of sine waves of TMS with wave frequency shown on the horizontal axis and wave amplitude on the vertical axis. To the right of each panel is shown an image of a magnetic resonance scan of a human head showing a sagittal (median) view of the brain with stylized TMS waves superimposed onto and aimed at the frontal section of the brain. Panel A shows TMS at a setting of 10 Hz at 120 percent of the motor threshold, the panel B TMS of 1 Hz at 120 percent of the motor threshold, and panel C TMS of 10 Hz at 110 percent of the motor threshold. The TMS settings and waves in panels A and B are shown in red, indicating that they did not yield success treatment outcomes, and the TMS setting in panel C is shown in green, indicating that it had good efficacy with very limited adverse effects.
Bad News
Dr. Diana's recruitment effort ran into a deep fund of suspicion. When Dr. Diana showed potential trial participants the TMS machine and explained its purpose, many accused him of intending to subject them to electroshock. Some declined to participate. In 2 years, he enrolled only 20 patients.
In mid-2015, Dr. Diana applied to the Italian Department of Anti-Drug Policies for an extension of his funding for the project. Weeks, then months, passed with no response. Dr. Diana's remaining funds from the past year dwindled. In July, he stopped recruiting patients because he was out of money to pay the laboratory to test hair samples for cocaine metabolites. He continued to provide his existing patients with psychological support and ask them about their cocaine use. Without biological confirmation, however, the scientific community would accord less weight to his patients' self-reports.
"Finally, in November, the Agency was forced to respond because I was making thousands of phone calls," Dr. Diana says. "I reminded them that we knew from the start this was going to be a 3-year project. It would be a shame not to finish, because we had encouraging preliminary findings. They told me, 'Look, we wish you all the luck you certainly deserve, but we don't have money to give you."
Striking the Tent
Unable to continue his study, Dr. Diana set out to reap what he could from his years of work.
He had administered real or sham TMS to 19 patients, far short of the 60 he needed to establish that his TMS approach was effective. "I can’t do any statistics on such a small number and hope to persuade my colleagues that our findings are predictive," he says.
Nevertheless, Dr. Diana says, "We didn’t have any choice. We had to either analyze our data and see what was there or just throw everything out." Although he could prove nothing with results from so few patients, at least he would find out if their outcomes were consistent with TMS being effective. If they were, his work might inspire others to try TMS.
The outcomes were indeed consistent. Patients in both the TMS- and sham-treated groups were using less cocaine 1 and 3 months after starting the treatment. The difference in the amount of reductions was not statistically significant, but a significant difference emerged at the 6-month follow-up. At that time, the patients in the TMS-treated groups were using about 70 percent less cocaine than they had before starting the trial, and the sham-treated group about 45 percent less.
In addition, Dr. Diana says, "The study participants commonly reported that their mood was much better. They were more comfortable with life. They didn't feel overwhelmed with guilt. Their anxiety levels went down significantly after the treatment. Some also described regularization of sleep, with better circadian rhythms."
For Dr. Diana, the persisting effect of TMS past 6 months hints that his most ambitious hope for TMS may pan out: The treatment may not just temporarily remit cocaine addiction, but actually restore the patient's brain to a pre-addicted state (see "Can Neurons Be Reeducated?").
Enthused and wishing to share his findings, Dr. Diana wrote a report to submit for publication. He knew the chances were slim that a journal would accept it. As of this writing, one journal has turned down the manuscript, and Dr. Diana awaits a decision from a second journal. (Update: In July 2016, Dr. Diana’s manuscript was accepted for publication in the journal Frontiers in Psychiatry−Addictive Disorders.)
Lessons and Plans
Dr. Diana sees his loss of funding in perspective. He notes that Italy is experiencing tight economic times and the government has reduced its investment in research: "We have a new prime minister who looks very efficient, very pragmatic. Everybody seems to be reporting that the country's situation is improving economically. But when you apply for funding for research, many times the answer you get is, 'We are now fixing things more important than research.' Unfortunately, they don't understand that it's through research and innovation that you generate more jobs and well-being for people."
Dr. Diana's broad perspective has not precluded disappointment. He says, "I worked on this study for five years. Before I even started to recruit patients, I worked 2 years to get it approved by the ethics committee and the hospital director, plus paperwork for this and that, endless paperwork. So it's very frustrating. But what can I say?"
Despite his disappointment, Dr. Diana remains excited about TMS. He has already teamed up with a collaborator, Dr. Giorgio Corona, in Cagliari, Sardinia. "We are set to continue this work and to replicate my observations with a larger sample," Dr. Diana says.
For Dr. Diana, starting over, although far from what he would have wished, presents opportunities to implement new knowledge and lessons learned. In his new trial, for example, he will measure patients' central dopamine levels, using a technique that came to his attention too late to be used in his previous trial (see "Windows Into the Brain").
The new trial's recruitment protocol will incorporate another lesson, this one learned at great cost: To put to rest misperceptions and mistrust, potential recruits will receive a thorough orientation designed to put them at ease about TMS. Dr. Diana says, "Our strategy will be to persuade patients that TMS really is safe and without side effects. We'll show them the machine. We'll show them videos of other people who have taken the treatment. And we'll tell them that if they perceive anything is wrong, they can leave the study whenever they decide."
Dr. Diana is eager to get his new trial underway. He says, "The idea that TMS can be useful has been reinforced in me. Comparing the effects we observed with TMS to what others are reporting with medications, I think TMS is the way to go. The new machine is being delivered as we speak."
Can Neurons Be Reeducated?
Dr. Diana explains, "We know from studies by Nora Volkow, Diana Martinez, and others that cocaine use over time weakens dopamine neurons. These neurons fire less often and less vigorously in the addicted brain, and this accounts for a person's cocaine craving and compulsive responses to cocaine cues. We administer TMS to increase those neurons' firing rate and strength back to their pre-cocaine levels. That might be therapeutic, but it won't be so great if the neurons just revert to their weakened state after the treatment, and the patient has to keep coming back indefinitely. We want an effect that lasts for a long time.
"Therefore our aim with TMS is to induce an effect called long-term potentiation, LTP, of the dopamine neurons. LTP is something that occurs naturally when a neuron repeatedly receives intense high-frequency stimulation from other neurons. The neuron develops structural changes that make it more active and sensitive to future stimulation, and that endure for extended periods.
"In my personal opinion, the results of my trial, although they are preliminary, indicate that TMS produced LTP of our patients' dopamine neurons. Our TMS-treated patients continued to use much less cocaine for 5 months after our 1-month treatment. The contrast in outcomes between our TMS-and sham-treated groups also supports this idea. We think that the sham TMS had a strong placebo effect that lasted 2 months after the treatment, possibly because the experience of sitting under the apparatus makes a powerful impression. After 5 months, however, the placebo effect began to wear off, while LTP kept the neurons in the TMS-treated group strong.'
Dr. Diana adds, "With TMS we were trying to tell the dopamine neurons, 'Okay. You fire faster, and remember that you are able to fire faster.' I think the neurons got the message."
Windows Into the Brain
The underlying idea of using TMS to treat cocaine addiction is that stimulation with magnetic pulses can re-invigorate hypofunctional dopamine signaling in the prefrontal cortex. To make the best case for TMS' efficacy, Dr. Martinez and Dr. Diana would like to show not only that TMS reduces cocaine use, but also that the reductions are paralleled by increases in dopamine. Retinography is a tool—albeit a tricky one—for accomplishing this. With retinography, researchers measure dopamine levels in the retina, and interpret them as indicators of levels in other parts of the central nervous system.