Network therapy—an office-based behavioral treatment that engages family and close friends in the recovery process—enhances abstinence among outpatients being treated with buprenorphine for opioid addiction. By the end of an 18-week NIDA-funded study, abstinence rates of patients who participated in network therapy (NT) were twice as high as those of a comparison group receiving standard medication management (MM) along with buprenorphine.
"NT transforms a few close relations from well-wishers to a team with skills to help patients achieve and maintain abstinence," says Dr. Marc Galanter, lead investigator of the study. In previous research, Dr. Galanter and his colleagues showed NT's promise as a therapy for cocaine addiction in both office- and community-based treatment settings; the new results in patients with opioid addiction add to the hopes that NT may offer a psychosocial adjunct to office-based buprenorphine treatment.
Dr. Galanter and colleagues at New York University Medical Center treated 66 heroin-addicted outpatients, aged 21 to 65, who reported abusing the drug for 12 years on average. Most (73 percent) had previous experience with addiction treatment, and about a third (30 percent) had tried methadone maintenance. Most lived with family or friends (77 percent) and were employed (67 percent). The investigators selected patients who could form a network—a few drug-free relatives or friends willing to help the patient achieve and maintain abstinence—and randomly assigned them to either MM or NT.
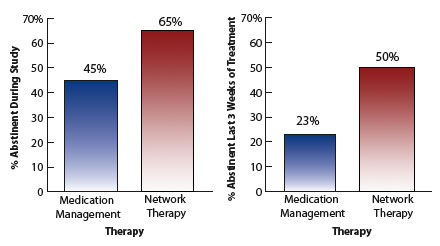 Network Therapy Increases Abstinence Among Patients Taking Buprenorphine. Among patients taking buprenorphine for heroin addiction, more of those who participated in network therapy attained abstinence during the 18-week study and throughout the last 3 weeks of treatment, compared with those who participated in medication management.
Network Therapy Increases Abstinence Among Patients Taking Buprenorphine. Among patients taking buprenorphine for heroin addiction, more of those who participated in network therapy attained abstinence during the 18-week study and throughout the last 3 weeks of treatment, compared with those who participated in medication management.All patients received a standard course of combined buprenorphine/naloxone tablets (16 mg/4 mg a day) taken under the tongue. Each patient also participated in two half-hour sessions per week of psychosocial treatment—either NT or MM—with a resident training in psychiatry. In MM, the therapist monitors the patient's response to the medication and encourages him or her to abstain from opioid abuse. The number of MM sessions and time investment are equivalent to those of NT, but the patient does not learn specific behavioral strategies for maintaining abstinence.
At the beginning of the study, patients chose people with whom they had an enduring relationship. Two people, on average, participated in each NT session with the patient. From the first NT session, therapists emphasized the primary guideline for this treatment approach: to focus on helping the patient achieve abstinence and to avoid discussions of relationship history, blaming, and emotional conflict. During sessions once a week, patients and their helpers communicated openly about events and people related to the patient's drug abuse and learned cognitive-behavioral techniques used widely in relapse prevention. As the supporters developed an understanding of relapse prevention, they helped the patient anticipate problem situations and develop recovery plans. They concentrated on creating an environment that helped the patient establish a drug-free residence, avoid substance-abusing peers, and stick to a medication regimen.
Although network members offer active support, patients in NT take full responsibility for their recovery. In weekly one-on-one sessions with a therapist, patients in the study strengthened the cognitive-behavioral skills they learned in network sessions, including monitoring of drug-abuse triggers, coping with craving, managing stress, and problem solving. Patients made and carried tools to assist them in recovery, such as cards to help them weigh drugs' attractions against the costs of abuse, written plans to deal with emergencies, and contact information for network members. The therapist encouraged patients to participate in 12-step programs, which can offer role models for abstinence and friendships with nonabusers. Throughout treatment, the researchers verified abstinence from illicit opioids with weekly urine tests.
Patients participating in MM and NT spent the same amount of time in therapy, 70 days on average, but more NT participants achieved abstinence by the end of treatment. Half receiving NT attained this goal, confirmed by opioid-free urine tests, during the last 3 weeks of treatment, compared with 23 percent of MM patients. More NT than MM patients produced opioid-free urine samples during the study (65 percent versus 45 percent). NT patients participated in 10 network sessions on average; those who attended more sessions sustained abstinence longer during the study. Whether the network comprised family or friends did not affect treatment outcomes.
An Office-Based Approach
"My colleagues and I designed NT principally for addiction treatment providers who do not have a large support team," Dr. Galanter says. "We find that those with psychotherapy experience learn the NT approach in about 10 training sessions with subsequent supervision." (See "Network Therapy Expands Treatment Capabilities of Small Practice Providers," NIDA NOTES, Vol. 18, No. 2)
"In this approach, a patient and therapist collaborate with a small group to achieve stable abstinence, weaving the contributions of each member and different treatment techniques into a supportive tapestry for a drug-free lifestyle. The network counteracts the environmental and social factors—for example, substance-abusing peers—that often compromise recovery," says Dr. Galanter. Although NT can help patients who have a few close associates willing to support their recovery, the therapy is probably not appropriate for homeless or mentally ill people or those who cannot achieve abstinence on their own for even 1 day.
Studies show that many heroin-addicted patients in treatment continue to abuse some form of opioids, with only about 20 percent of those on buprenorphine medication demonstrating opioid-negative urine tests at the end of 1 month of treatment. Extending the therapy to 2 to 6 months increases the percentage of opioid-negative urine tests to 50 to 60 percent. Dr. Dorynne Czechowicz of NIDA's Division of Clinical Neuroscience, Development and Behavioral Treatment says, "It's impressive that NT therapy enhanced the results typically seen with short-term buprenorphine medication." She emphasizes that the researchers should examine whether NT reduces abuse of other drugs among opioid-addicted patients, particularly cocaine, which puts people who are in recovery at high risk for opioid abuse relapse. She adds that investigators should also conduct longer-term studies to determine whether patients maintain these treatment gains and demonstrate NT's effectiveness in general medical practice.
Dr. Galanter and his colleagues have posted a brief introduction to NT on the Internet (http://www.med.nyu.edu/substanceabuse/manuals/nt/). The American Psychiatric Association sells a training video on NT as an office-based addiction treatment; the video is appropriate for any mental health professional.
Source
- Galanter, M., et al. Network therapy: Decreased secondary opioid use during buprenorphine maintenance. Journal of Substance Abuse Treatment 26(4):313-318, 2004. [Abstract]